

A doctor’s education classically begins with an introduction not to the living but to the dead. And so it was for me some forty years ago. After the opening lecture on human anatomy in a large amphitheater, our class moved to a cold subterranean room. There, scores of cadavers covered by plastic sheets lay on stainless steel tables. The pungent smell of formaldehyde filled the cavernous space.
We were divided into groups of four, each group assigned a body. As a fellow student lifted the plastic sheet, I saw a female of indeterminate age with bronze-colored skin, a taut belly, and puckered breasts. Age was hard to ascertain because the bodily features we focus on to recognize individuals—face and hands—were covered in tightly wrapped gauze. The instructor directed our attention to the arm, and I made a tentative first cut with a scalpel to open the skin and expose the biceps muscle. Over the ensuing weeks, we marched across the limbs, meticulously dissecting muscle and nerve and tendon, tying fine strings around each isolated part with a small tag to identify the structure. Ultimately, we reached the boundaries of the exposed skin, and were told to remove the gauze coverings. My cadaver’s head was crowned by matted gray hair and her hands were fine and boney, the knuckles distorted by arthritis. We made precise incisions and exposed the muscular splay of the palm.
It was a late autumn afternoon when we completed the dissection, and as I walked along Fort Washington Avenue to the dormitory, I glanced down and saw something on the toe of my shoe. At first I didn’t know what it was, and then realized that a thick clump of flesh had fallen from my cadaver. I stood motionless for a long while. I felt as if I had committed a sacrilege, violated a boundary, by removing the dead from a proper hidden place.
I thought how the cadaver was intentionally masked so as not to be a person. And how the dead were distant to me. No one I knew had died, and I had never been to a funeral. My mind in the dissecting room had been fully occupied with recognizing the shapes and locations of anatomatical parts. Now, I was gripped by the sense that I must be much more than simply these parts, that I had a dimension distinct and above the physical. But might the reductionists be right? Was I in the end merely a mass of interacting molecules, and my sense of self, the conscious perception of an existence beyond the material, an illusion?
The anatomy laboratory was locked after each dissection, so I slowly retraced my steps, careful not to dislodge the piece of flesh, back from Fort Washington Avenue to a small garden behind the medical school. There, I took a leaf and detached the fragment and then covered it with a thick layer of earth.
That was the first time medicine had brought me close to mystery. And over the ensuing decades as a physician, I experienced more such moments, as an intimate witness to life’s great mysteries: the sudden arrival of new life at birth; the perplexing passage to death; the desperate desire of patients to find meaning in illness. Did each moment offer a glimpse of the soul, its arrival, its departure, its struggle? And what might a physician learn from those times about his own life?
Victoria Sweet opens God’s Hotel, a beautifully written and illuminating book, with an experience of wonder similar to mine. She is not in the anatomy lab but in the autopsy suite, and recognizes a patient, Mr. Baker, whom she had treated:
I watched as the pathologist set to work with his electric saw. He opened the chest wall and removed the soggy, honeycombed lungs. He weighed them each separately, first the right lung, then the left. Then he took out the large and heavy heart, with its right side hypertrophied from lung disease, and documented its weight in grams. Next he opened the abdomen and ditto the liver, the spleen, the pancreas, the kidneys. Each organ was removed and weighed, and its weight in grams tallied. The blood vessels, large and small, were inspected and commented upon. Then the saw attacked the head. Sure enough, there it was—the brain—looking just like it did in the books, gray, spongy, with a texture kind of like pâté—homogeneous, boring. Then Mr. Baker was done. We were done. Finished. That was it. Nothing more inside.
Sweet then explains why this experience left her “strangely disappointed.”
There was nothing else to see. No hidden place, unexplored and unexplorable, no unopenable, small black box, hidden in all those wiggly intestines. It was undeniable—Mr. Baker had completely disappeared. Autopsied, his body was nothing more than a suit of clothes lying disregarded in the corner.
Something was missing. But what? Mr. Baker’s breathing? His movement? His warmth? What I had expected, I later came to realize, was some sort of thing, some unopenable last nubbin, like what you find at the center of a baseball when you unroll it. I had expected some thing that was, well, ineradicably Mr. Baker, something the pathologist’s saw could not open and destroy. But there was no such thing; I could see for myself.
What might the thing be that Sweet expected to find? Deeply grounded in Christian concepts, she writes that the Latin spiritus, from which we get the English “spirit,” was not as insubstantial as “spirit.” “Spiritus was the breath, the regular, rhythmic breathing of the live body that is so shockingly absent from the dead. Spiritus is what is exhaled in the last breath.”
Advertisement
Sweet’s Latin exegesis can be traced back to the Genesis narrative of human creation. “Adam” comes from the Hebrew word for earth, how human life began when God breathed into the dust of the earth. The term for “spirit” is ruach in Hebrew, a synonym for wind, and “soul” is neshama, derived from the word for “breath.”1
But what Sweet ultimately seeks is anima, a life force with an Aristotelian resonance:
And there was anima. Usually translated as soul, the Latin is better for conveying the second striking distinction between Mr. Baker’s dead body and Mr. Baker—its lack of movement. Because anima is not really the abstraction, “soul.” Anima is the invisible force that animates the body, that moves it, not only willfully but also unconsciously—all those little movements that the living body makes all the time. The slight tremor of the fingers, the pounding of the heart that shakes the living frame once a second, the gentle rise and fall of the chest. Those movements by which we perceive that someone is alive. Anima, ancient medicine had observed, is just as absent from the dead body as spiritus.
As with many doctors with a liberal education, Sweet’s pondering of philology and philosophy recedes in the presence of physiology and pharmacology. Her daily tasks are clinical, where science prevails:
During all those years I was ever more impressed by the power of modern medicine—by its logic, its method for arriving at a diagnosis and a treatment. Yet every now and again I had other experiences like that with Mr. Baker—experiences that left me wondering…. All evidence of some subtle but shared world, where beings popped up and disappeared, of invisible connections with visible effects.
Victoria Sweet served as a physician at Laguna Honda, the last almshouse in the city of San Francisco, and perhaps in the country. Its French equivalent was Hôtel Dieu—God’s Hotel. Supported by the city of San Francisco, Laguna Honda accepted all in need, or as Sweet puts it, those who had “no other place to go.” Of course, there were other places where they had been: on the streets, sleeping in cardboard boxes or beneath highway underpasses, or in filthy tenement apartments and SROs, where they were neglected or abused, or abused themselves through drugs and alcohol.
Such patients typically are the bane of interns or residents, depicted in Samuel Shem’s The House of God (1978), a roman à clef about a Boston teaching hospital. In that novel, read by virtually every doctor I’ve known, Shem charted the trajectory of the many interns who arrive idealistic, with a humanistic vision of medicine, and end their first year of training bitter, cynical, depressed, and mercenary. The word used by Shem’s young doctors for the elderly demented and debilitated patients is “GOMERs” (Get Out of My Emergency Room). The doctors feel that they can’t do anything for the GOMERs. (They should be “turfed,” transferred out of your charge as quickly as possible.)
God’s Hotel is the counterpoint to The House of God. Instead of becoming alienated from those who arrive in old filthy clothes, malnourished, confused, or delusional, Sweet draws ever closer to them. She takes on each case looking for clinical clues about an underlying problem whose remedy might improve the patient’s condition. For example, in one chapter where she oversees a ward populated by the demented, Sweet does not blithely accept the convenient label of Alzheimer’s disease that was fixed onto her charges. Rather, she looks for conditions like abnormal thyroid function or B12 deficiency and especially overmedication with antipsychotic drugs or tranquilizers that could explain the blank faces and slurred words and episodes of delirium. Occasionally she discovers such remediable problems, and restores a patient to an aware and meaningful life.
Advertisement
In her acknowledgments Sweet thanks Oliver Sacks as an early reader who encouraged her, and she expands on the approach that Sacks took in An Anthropologist on Mars (1995). Sacks’s focus is on adaptation; he seeks to understand how each person’s clinical condition connects with his or her environment. He journeys to the home of a physician with Tourette’s syndrome and to the workplace of Temple Grandin, a veterinary scientist with Asperger’s syndrome. Victoria Sweet is also an anthropologist of sorts, but one who explores the unique environment of Laguna Honda.
At this hospital there are antibiotics and anti-arrhythmics, surgeons and radiologists, the latest technology and treatments. But its world sharply differs from what we know as “modern medicine” not only in space, with large open wards, but in time. There was no imperative to diagnose and treat a patient quickly, no administrator trolling through the wards checking “length of stay,” a merciless metric that pushes patients out the door so that the institution is paid well. Rather, as Sweet describes, there was “slow medicine,” time to observe and think. Ironically, as she repeatedly shows, patients sent to Laguna Honda after having been “turfed” by desperate doctors elsewhere received better care than could be given in other clinical settings. Sweet argues that the worlds these people inhabit are destructive and daunting, too difficult to meaningfully change. What is needed then is sanctuary, a safe place, where they are protected from the pimps who beat them and the landlords who shut off their heat, the thieves who steal their welfare checks, the drug dealers who supply their habits, and the families who neglect them.
Several years ago, I cared for a woman with breast cancer. Her treatment began with surgery and radiation for the initial tumor, and then a series of chemotherapeutic drugs, each inducing only a temporary remission. Ultimately, the cancer grew in her liver and bones. I knew of no drugs, either standard or experimental, that offered a real chance of ameliorating her condition. Early in the evening when the hospital grows quiet, I went to her bedside to tell her.
I sat and grasped her hand and described how the cancer had regrown. “Barbara,” I said, “we’ve been honest with each other every step of the way. I know of no medicines that I can give at this point to help you.” For a long while we sat together in heavy silence, and then she turned to me and shook her head, “No, Jerry. You do have something to give. You have the medicine of friendship.”2
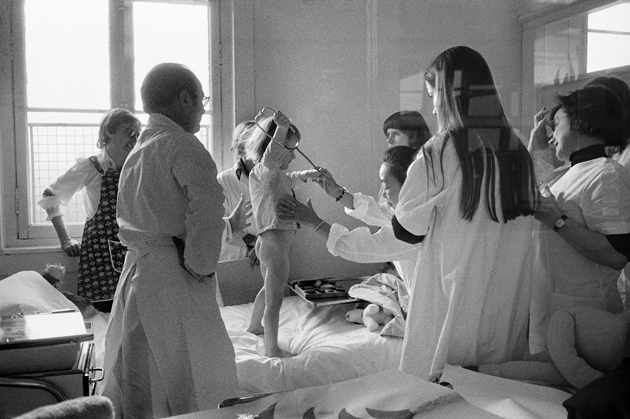
Victoria Sweet describes how one patient early in her career taught her about this other dimension of a doctor’s care:
Miss Tod capped my experience of those first years at Laguna Honda. She summarized it and hinted at what I would be learning later. Even when there is nothing to do for a patient—no cancer to discover, no paradoxical pulse to take—there is still something to do. It doesn’t have to be lifesaving, grandiose, and heroic. It can be as simple as a pair of glasses or a different diet. In fact, it usually is.
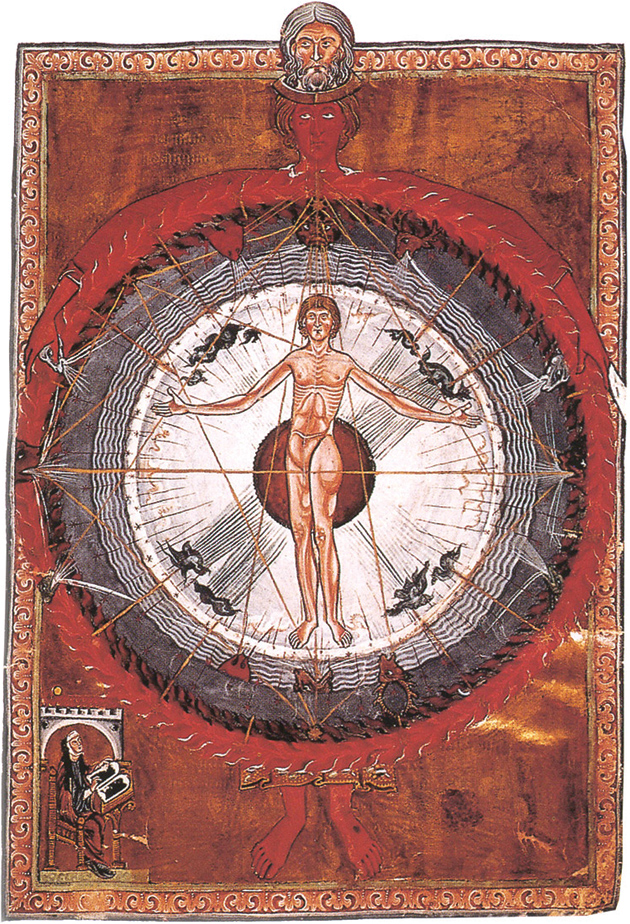
Sweet later decided to work part-time at Laguna Honda, so as to pursue graduate study in the history of Western medicine. She chose as a thesis topic the work of Hildegard of Bingen, a nun who lived in the twelfth century, a mystic, composer, and theologian, as well as a medical practitioner. She wrote a book about diagnosis and treatment. Sweet writes, “Although [it] was not a great book, it was thrilling.” The thrill was that it emphasized the observation of the ill, and the importance of focusing on their environment. Hildegard’s medicine did not imagine the body as a machine or disease as mechanical breakdown. Rather, as Sweet elaborates, Hildegard had a
remarkable concept of viriditas. Viriditas comes from the Latin word for green, viridis—which also gives the French vert, and the Italian and Spanish verde. Viriditas meant greenness. So usually it referred to the color of plants or of gems like emerald, although it was also used metaphorically to mean vigor or youthfulness.
But Hildegard used viriditas—greening or greenness—in a broader sense…. She used it to mean the power of plants to put forth leaves, flowers, and fruits; and she also used it for the analogous power of human beings to grow, to give birth, and to heal.
Hildegard’s metaphor informs Sweet’s therapeutic approach to Terry, a patient at Laguna Honda with an open bedsore, festering with microbes that were mercilessly feasting on the decaying flesh. This was not a small, simple bedsore, but a cavernous wound that extended to the surface of bone and had dramatically worsened at other hospitals:
To see what else was needed, I had to start with a vision of Terry whole, complete, and healthy, in a future when all that was missing from her complete health was a pair of glasses. And walk my way back from that. Which I did. I walked past the repair of her teeth, the strengthening of her body, the strengthening of her will, the resolution of her depression, and the healing of her bedsore. I walked all the way back from the perfect future to the imperfect now, and then I organized my strategy forward.
What my strategy would be, I understood from Hildegard, was that in addition to removing obstructions to viriditas, I would fortify Terry’s viriditas with Earth, Water, Air, and Fire. That is, with good nutrition—tasty food, vitamins, liquids—deep sleep, fresh air, and sunlight.
After that? Peace. Rest. Safety.
Not much else. It might be just that simple. Oh, and time. As much time as Terry needed.
This approach succeeds, and affords a lesson not only for this one patient but for our health care policymakers:
With Terry, I witnessed healing from the inside out…. What was ironic was how difficult it was for her to get it. Our much-criticized health care system provided every medication, no matter how expensive, and every necessary procedure; and yet, after each of her fifty-thousand-dollar hospitalizations, she was discharged in a wheelchair to the streets or the Baxter Hotel. The value of Laguna Honda, where time was not at a premium, struck me. Patients like Terry should, I decided, be tucked away at our hotel, out of sight of the administrators and out of the mind of budgeters, so the tincture of time could do its work.
But it was watching her healing that was miraculous, that transformed my practice of medicine. In this day of efficient health care, no one ever gets to see such a process. It seemed to me more than mechanical; it seemed magical, a sleight of hand.
Sweet is not a Luddite; her metaphors are poetic and hint at the mystical, but she then pulls back with the educated eye of a scientist:
Of course, modern medicine can readily explain the mechanism of Terry’s healing. Once the breeding tissue for microbes had been removed by our plastic surgeon and nutrients provided, healthy cells at the base of the wound dedifferentiated—that is, they lost various inhibitive structures on their DNA. They turned into pluripotential stem cells, and then, by means of a complex but explainable process of membrane receptors, enzymes, and transcriptases, they began to produce first the RNA and then the proteins necessary for reconstituting the muscle cell, the endothelial cell, the cartilage cell, the collagen. There was nothing magical about it. Once this process was set in motion, it happened mechanically.
And yet it felt like something different, as if I were watching an invisible artist fill in his vision of Terry Becker’s perfect body. I wouldn’t say that modern medicine was wrong in its explanation, but the process seemed more than mechanical; it seemed deliberate, as if there were a perfecting force, clear about its purpose and its final form. But, just like the absence of the little black box at Mr. Baker’s autopsy, I had no word for it….
Watching Terry heal from Hildegard’s perspective of viriditas changed my point of view…. Forever after, instead of focusing on my patient vaguely surrounded by his environment, I also did the opposite—I stepped back and focused on the environment surrounding my patient. And asked myself: Is anything interfering with viriditas? What can I do to remove it?
Sweet’s study of medieval medicine, its concepts expressed in Latin and Greek terms, informs not only her unique view of clinical care, but her evolving sense of self:
Physis—the individual nature of each person—also gives us the word physician. The physician is the person who studies physis, the individual nature of his patient, who understands it and follows its lead.
She also draws on her experience making a Catholic pilgrimage in southern France and Spain, offered hospitality in convents and monasteries, to illuminate a contranym:
The essence of hospitality—hospes—is that guest and host are identical, if not in the moment, then at some moment. Whatever our current role, it was temporary. With time and the seasons, a host goes traveling and becomes a guest; a guest returns home and becomes a host. That is what the word hospitality encodes. And in a hospital, the meaning of that interchangeability is even more profound, because in the hospital, every host will for sure become a guest; every doctor, a patient.
Ultimately, Sweet and her fellow physicians and nurses at Laguna Honda are buffeted by the powerful forces reconfiguring American health care in the form of efficiency experts, politicians, budget directors, and government lawyers. The culture of an institution where time is not limited cannot persist. Indeed, its space also is changed, as a new building is erected. But even as the environment changes, Sweet still experiences instructive moments, like the “return” of Meng Tam, a patient who had been designated “DNR,” for “do not resuscitate.” Tam’s heart was diseased and entered into ventricular fibrillation, a lethal arrhythmia in which blood cannot be effectively pumped to the tissues:
We looked at each other, and Hildegard’s lines about dying came into my mind: “It is as if the soul, the anima, stands with one foot in this world and one in the next, uncertain whether to stay or go.” That was just it. Meng Tam was undecided. He was halfway between life and death. And as I looked into his eyes, which were soft, shining, almost a greenish color, I saw them become clear and still, like a shallow mountain pool after a rain, and I knew that he had decided to stay. I can’t tell you that I nodded, but I knew, and Meng Tam knew that I knew, that he was coming back.
But the DNR order does not allow Tam to be electro shocked into a normal cardiac rhythm, or intubated. Sweet and her colleague Dr. Mark revert to ancient measures:
I called Meng Tam’s name, and I shook him, and Dr. Mack started to move his legs. I even slapped his face a few times. And sure enough, Meng Tam’s pulse returned; it became quite steady; and then his eyes opened and stayed open, staring at me….
In my first autopsy I’d been surprised by the difference between the dead body and the live Mr. Baker I’d known. There was something missing—that I missed, and that I’d missed. And now with Mr. Tam I’d caught it; seen it go toward death, stop, change its mind, and come back. I’d seen the anima—that which animates the body and the mind.
A reader, medical professional or not, may not embrace all of Sweet’s visions, expressed in the metaphors of Hildegard. Nor must one have a religious sensibility, specifically a Catholic one, to appreciate her insights. For both agnostic and believer, Sweet pinpoints the element of medicine that makes it a calling rather than a job: the unique and sustaining love that is sparked between doctor and patient or nurse and patient. This love opens up an avenue for understanding the patient as a person rather than as a body with disease. Love does not occur with every person you care for, nor is it felt at every moment for those who are special to you. But it may be felt acutely at those moments of mystery, at birth and at death, and during a patient’s struggle to find meaning in her condition. Indeed, it is the ultimate antidote to suffering, given without prescription. And as with all forms of love, it enriches the life of not only the recipient but the giver.
This Issue
September 27, 2012
Pride and Prejudice
Cards of Identity
Are Hackers Heroes?
This Issue
September 27, 2012
Pride and Prejudice
Cards of Identity
Are Hackers Heroes?
-
1
Islam uses similar Arabic terms: al-Nafs is the soul, with Nafas meaning “breath”; al-Ruh is the spirit, related to “wind.” The Ruh and the Nafs are both inexorably linked to the physical body, yet remain distinct from it. At the moment of death, they break this bond by leaving the body, which is described like a thorn being pushed through a cloth—the cloth resists and strains for a moment, then the thorn suddenly pierces clean and free through it. ↩
-
2
Jerome Groopman, The Anatomy of Hope (Random House, 2004), p. 135. ↩

{kind=link}
{kind=link}